Dry eye disease affects an estimated 16 million Americans, with many more experiencing symptoms without a formal diagnosis. Understanding the root causes of this multifactorial condition starts with examining the delicate structure that protects and nourishes the eye’s surface – the tear film.
Your Tear Film’s Three Critical Layers
The tear film is a complex structure composed of three distinct layers, each serving a vital function in maintaining healthy vision and comfort. The outermost lipid (oily) layer is produced by the meibomian glands located in the eyelids. This layer prevents tear evaporation and creates a smooth optical surface needed for clear vision. When functioning properly, it acts like a protective seal, keeping moisture locked in.
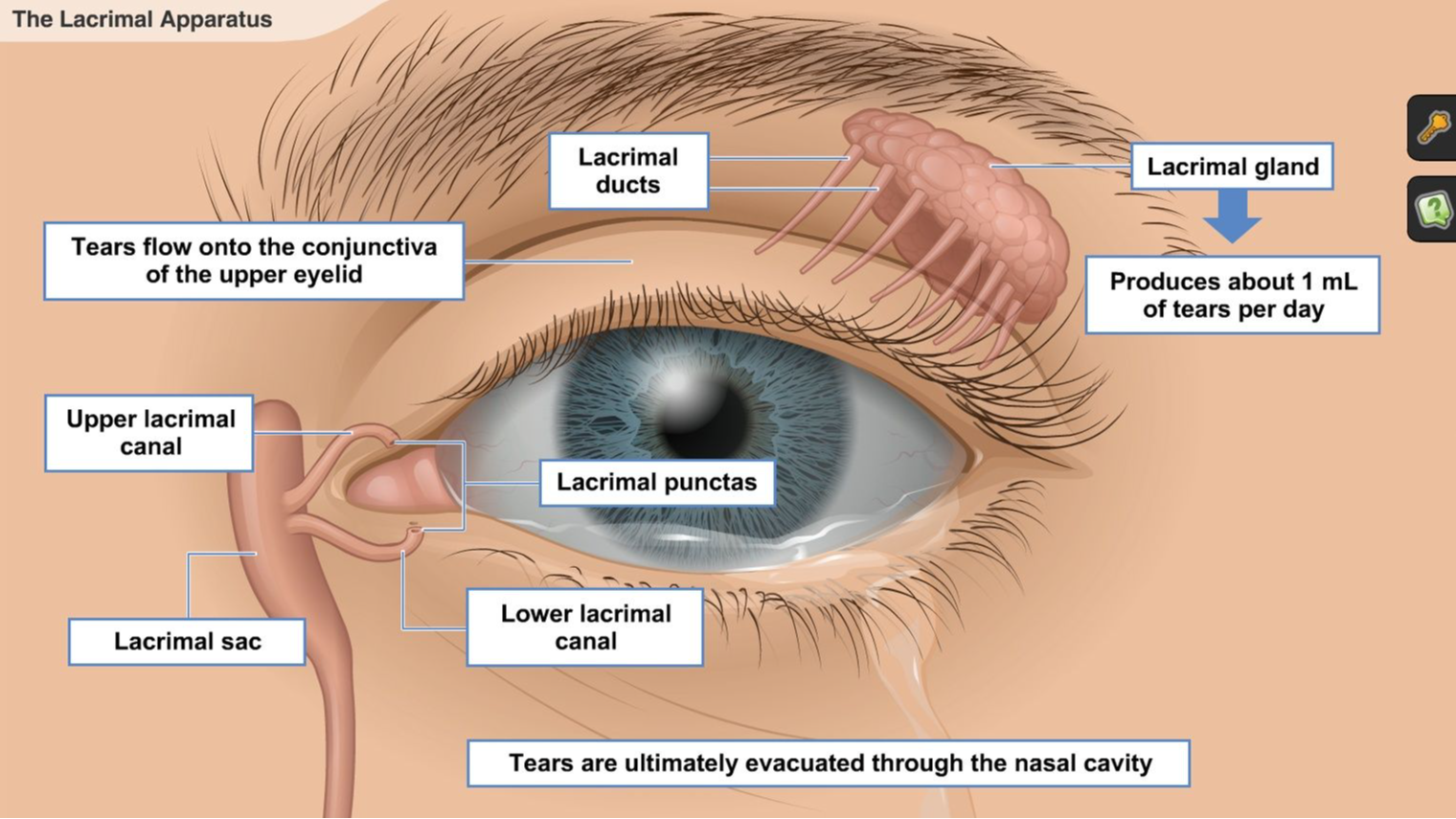
The middle aqueous (watery) layer makes up the bulk of what people recognize as tears. Secreted by the lacrimal glands, this layer provides oxygen and nutrients directly to the cornea while washing away debris and foreign particles. It’s the workhorse of the tear film, constantly refreshing and cleansing the eye’s surface.
The innermost mucin (mucus) layer is produced by goblet cells in the conjunctiva. This layer helps spread the aqueous layer evenly across the entire ocular surface, allowing tears to adhere properly to the eye. Without adequate mucin, tears would simply roll off the eye rather than providing protection and lubrication.
Common Causes of Tear Film Disruption
1. Meibomian Gland Dysfunction (MGD)
Meibomian gland dysfunction represents the leading cause of evaporative dry eye, affecting the vital lipid layer. When these oil-producing glands become blocked or produce abnormal secretions, tears evaporate too rapidly from the eye’s surface. The blockages often result from thickened oils that can’t flow properly, creating a domino effect of discomfort.
MGD commonly develops due to factors like hormonal changes, certain medications, or chronic eyelid inflammation. Patients typically experience a gritty sensation, burning, and fluctuating vision that worsens throughout the day as tear evaporation accelerates. The condition often coexists with blepharitis, creating a cycle of inflammation and gland dysfunction.
2. Insufficient Tear Production
Aqueous-deficient dry eye occurs when the lacrimal glands fail to produce adequate amounts of the watery layer. This type of dry eye is particularly common in individuals with autoimmune conditions like Sjögren’s syndrome, where the body’s immune system attacks moisture-producing glands. Age-related hormonal changes, especially in post-menopausal women, also significantly impact tear production.
Certain medications can reduce tear production, including antihistamines, decongestants, blood pressure medications, antidepressants, and hormone replacement therapy. The resulting tear deficiency leaves the eye’s surface vulnerable to damage and creates the characteristic symptoms of dryness, irritation, and visual disturbance.
3. Environmental and Lifestyle Factors
Modern lifestyle factors play an increasingly significant role in tear film disruption. Prolonged screen time reduces blink rates by up to 60%, preventing proper tear distribution across the eye’s surface. Air conditioning, heating systems, and low-humidity environments accelerate tear evaporation, while exposure to wind, smoke, and pollutants can irritate the ocular surface.
Contact lens wear can disrupt all three tear film layers, particularly with extended use or poor lens hygiene. Refractive surgeries like LASIK can temporarily affect corneal nerves that regulate tear production. Additionally, nutritional factors, including omega-3 fatty acid deficiency, may impact the quality of the lipid layer.
Recognizing Dry Eye Symptoms
Primary Warning Signs
Dry eye symptoms extend beyond simple dryness, often manifesting as a constellation of uncomfortable sensations. Patients frequently describe a foreign body sensation – feeling like sand, grit, or an eyelash is stuck in the eye. Burning and stinging sensations are common, particularly in windy conditions or dry environments.
Visual symptoms include blurred or fluctuating vision that improves with blinking, light sensitivity (photophobia), and difficulty with tasks requiring sustained visual attention, like reading or computer work. Eye redness, especially along the eyelid margins, often accompanies these symptoms. Mucoid discharge may accumulate, particularly upon waking.
Why Eyes Water When They’re Dry
One of the most confusing aspects of dry eye is paradoxical tearing – excessive watering in response to dryness. This occurs when the inadequate baseline tear film triggers the lacrimal glands to produce reflex tears in large quantities. However, these reflex tears are primarily composed of the aqueous layer and lack the proper balance of oils and mucins needed for stable coverage.
The result is a cycle where excess watery tears provide temporary relief but quickly evaporate, leaving the eye even drier than before. This explains why patients often report watery eyes that feel dry and uncomfortable – the tears themselves aren’t providing effective lubrication.
Professional Diagnosis Methods
Eye Examination
According to ophthalmologists at Clear Vision Ophthalmology in New York, professional diagnosis begins with a detailed symptom assessment and a thorough eye examination — evaluating eyelid position and function, the quality and quantity of tears, and the overall health of the ocular surface. The examination includes checking for signs of inflammation, evaluating blink patterns, and identifying any underlying conditions contributing to symptoms.
A thorough medical history reveals important information about medications, systemic health conditions, environmental exposures, and lifestyle factors. Practitioners also assess symptoms using standardized questionnaires that help quantify the impact on daily activities and quality of life.
Specialized Tear Film Tests
Several diagnostic tests provide objective measurements of tear film function. The Schirmer’s test measures tear production by placing small paper strips along the lower eyelid to absorb tears over a five-minute period. Results below 10mm of wetting typically indicate insufficient tear production.
Tear breakup time (TBUT) testing evaluates tear film stability by measuring how quickly the tear film breaks apart after a complete blink. Fluorescein dye is instilled, and the time until dry spots appear is measured under magnification. Normal TBUT exceeds 10 seconds, while values below 10 seconds suggest evaporative dry eye.
Additional specialized tests may include tear osmolarity measurement, which detects the salt concentration in tears, and matrix metalloproteinase-9 (MMP-9) testing, which identifies inflammatory markers on the ocular surface. These objective measurements help determine the specific type and severity of dry eye disease.
Evidence-Based Treatment Options
First-Line Treatments
Initial management typically begins with preservative-free artificial tears used frequently throughout the day. These lubricating drops supplement natural tears and provide immediate symptom relief. For nighttime dryness, thicker gels or ointments offer longer-lasting protection while sleeping.
Warm compresses applied for 10-15 minutes help liquefy thickened oils in the meibomian glands, improving lipid layer function. Eyelid hygiene using specialized cleansers reduces bacterial populations and inflammation along the eyelid margins. Environmental modifications include using humidifiers, avoiding direct air currents, and wearing wraparound glasses outdoors.
Lifestyle adjustments play a vital role in symptom management. Taking frequent breaks during screen time, practicing conscious blinking exercises, and staying well-hydrated support natural tear production. Omega-3 fatty acid supplements may improve oil gland function and reduce inflammation.
Prescription Medications
When over-the-counter treatments prove insufficient, prescription medications target the underlying inflammatory processes. Cyclosporine eye drops (Restasis, Cequa) are immunomodulatory agents that reduce inflammation and increase natural tear production. These medications typically require 6-12 weeks of consistent use to achieve maximum benefit.
Lifitegrast eye drops (Xiidra) block specific inflammatory pathways involved in dry eye disease. Some patients experience improvement within 2 weeks, though full effects may take several months. Perfluorohexyloctane drops (MIEBO) represent a newer approach, creating a protective barrier that prevents tear evaporation without containing water.
Short-term topical corticosteroids may be prescribed during acute flare-ups to rapidly reduce inflammation. However, these require careful monitoring due to potential side effects, including increased eye pressure and cataract formation with prolonged use.
Advanced Procedures
Punctal plugs offer a mechanical approach to dry eye treatment by blocking the tear drainage ducts, allowing natural and artificial tears to remain on the eye’s surface longer. These tiny silicone or gel devices can be inserted in-office and are reversible if complications arise.
For severe meibomian gland dysfunction, thermal treatments like intense pulsed light (IPL) therapy or specialized heating devices (TearCare, LipiFlow) help restore proper gland function. These procedures use controlled heat and expression to clear blocked glands and improve oil flow.
Advanced cases may require autologous blood serum drops, created from the patient’s own blood plasma. These drops contain growth factors and nutrients that promote ocular surface healing. Amniotic membrane transplantation provides biological scaffolding for severe surface damage, while scleral contact lenses create a protective reservoir of moisture for end-stage disease.
When To See an Eye Doctor
Effective dry eye management starts with an accurate diagnosis and a treatment plan tailored to your specific symptoms and underlying causes. Early intervention matters — without it, the condition can progress to more serious complications, including corneal scarring, ulceration, and vision impairment. Because dry eye is multifactorial, treatment often involves a combination of approaches and may need to be adjusted over time to achieve lasting relief.
Treatment success depends on identifying which tear film layers are compromised and addressing both symptoms and root causes. Patients should expect improvement to occur gradually, with some treatments requiring weeks to months for full effectiveness. Regular follow-up appointments allow for treatment modifications and monitoring for potential complications.
CLEAR VISION OPHTHALMOLOGY PLLC
79-10 34th Ave
Suite 1Y
Jackson Heights
New York
11372
United States